Ankle Sprains and Instability
What is it?
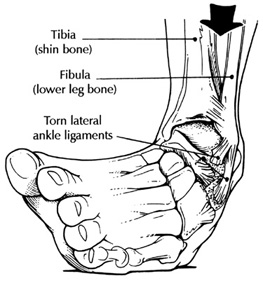
A sprain is an injury to the ligaments around the ankle and occur when you 'roll' the ankle over. The ankle is the joint between the leg and the foot, and serves as a hinge for the foot to rotate around. It is made up of the Tibia, Fibula and Talus bones and the joint is held in place by bands of tissue known as ligaments. The outside of the ankle has three ligaments (lateral ligament complex) and it is the front band (anterior talo-fibular ligament "ATFL") that is most commonly injured during a sprain. The deltoid ligament is on the inside of the ankle and is much stronger - this will be torn in a severe sprain. Just above the ankle joint, there are even stronger ligaments securing the tibia and fibula together, which may be injured during severe sprains or fractures.
What Causes Sprains?
During a sprain there is over-stretching of the tissues causing tears to the ligaments, with pain, swelling and later bruising.
However, if further force is applied to the ligament, it may rupture, or event to pull off a flake of bone from the ligament attachment point (avulsion fracture).
The body's natural reflex is to prevent the ankle turning, by contraction of the peroneal muscles. A sprain places them under excessive strain and this can split, tear or dislocate the tendons, or even 'pull off' (avulse) the bone they insert onto (5th Metatarsal avulsion fracture).
In more severe injuries, as the ankle rolls or turns, the bones of the ankle joint (Talus, Tibia & Fibula) are tilted forcibly within the joint. This causes either a bruise of the cartilage and bone, or a chip of the cartilage (osteochondral defect "OCD") is knocked off.

Xray showing Tibia, Fibula and Talus.
Stress views revealing severe instability
Ankle sprains are the most common musculoskeletal injury with an estimated 6,000 ankle sprains each day in the UK. Most will get better with the standard RICE (Rest Ice Compression Elevation) treatment after 1-2 weeks.
However, in the more severe cases, 30% of patients will go on to have chronic symptoms of either pain or instability. Therefore, if there has been little improvement after 2 weeks or symptoms continue at 6 weeks, then a review by an Orthopaedic Foot & Ankle Surgeon is recommended.
Diagnosis
From the history of the injury, and a description of the symptoms, a specialist will be able to diagnose the sprain.
The most common problems following a sprain are: continued swelling, continued pain, catching or locking of the ankle or instability with the ankle giving way.
Swelling
This is very common and part of the healing process, it will takes weeks or months to settle in major sprains. If it does not gradually improve or is associated with pain, it will be due to damage to the ankle joint and should be investigated.
Pain
This normally settles and certainly should be much improved or complete gone within 6 weeks. If it continues or is not improving, then it should be investigated.
Catching / Locking
This is a sensation that there is something trapped or moving in the joint and the joint may actually get 'locked' where no movement is possible. It is usually painful but does not have to be. This should be investigated.
Painless grinding of the joint or Crepitus, is quite common following these injuries and does not require any treatment. It usually settles of its own accord.
Instability
This is when the ankle 'gives way' regularly. It is usually do to weakness of the muscles that control the ankle and responds very well to physiotherapy. It may be due to overstretching of the ligaments or an OCD of the ankle joint. If there is not a rapid improvement with physio then this should be investigated.
Treatment
Most sprains recover naturally with rest within a few days. For more serious sprains however, where the patient is unable to place any weight upon the ankle, a course of physiotherapy designed to restore normal function to the ankle, while simultaneously strengthening, and improving co-ordination of the muscles that serve to stabilise the ankle. The co-ordination, known as proprioception, may need to recover as the nerve endings in the ankle may become damaged in the case of a severe sprain. (Click here for link to ankle sprain exercises).
If the ankle does not recover even after intense physiotherapy, and the pain & deformity persists for 6 weeks, it is advisable to have the ankle fully assessed with an MRI scan.
In those circumstances where the ankle repeatedly gives way under pressure (known as a repeated inversion injury), then surgical options can be explored. A detailed examination is undertaken to identify any unoticed fractures, tendon injuries or nerve problems.
Where inflammation does not respond to conservative measure, steroid injections may prove effective. Although MRI & CT scans are extremely good at identifying the underlying causes, in some cases ankle arthroscopy performed to investigate the ankle joint and articular surface of the talus. (Click here for link to Ankle Arthroscopy)
Surgery will involve the reconstruction the lateral ligaments, either by directly repairing the damaged ligaments, or the excision and transplant of a tendon from the back of the ankle. Following this surgery, the ankle will have to be immobilised for 6 weeks, followed by a course of physiotherapy. (Click here for information on ankle ligament reconstruction surgery).
In the severe or chronic sprain, it is very important that the whole ankle is fully assessed, looking for these other injuries. A careful and precise assessment will usually identify the most likely injury, and is further confirmed with specialised ultrasound scans or MRI scans. This will usually identify the cause of the continued symptoms.