MTP Joint Fusion

Arthritis of the big toe joint (first metatarsophalangeal or MTP) causes disabling pain and swelling. Arthritis develops when the cartilage, which acts as the cushion and lubricant in the joint, wears away and the bones on either side of the joint rub against one another. As the arthritis progresses, large spurs form around the joint and especially on top. This causes the classic “Dorsal Bunion”. The arthritis causes the joint pain and the spurs cause pain from rubbing in shoes - eventually it becomes impossible to find any shoes that fit! The joint will often become very stiff and even rigid from the arthritis.
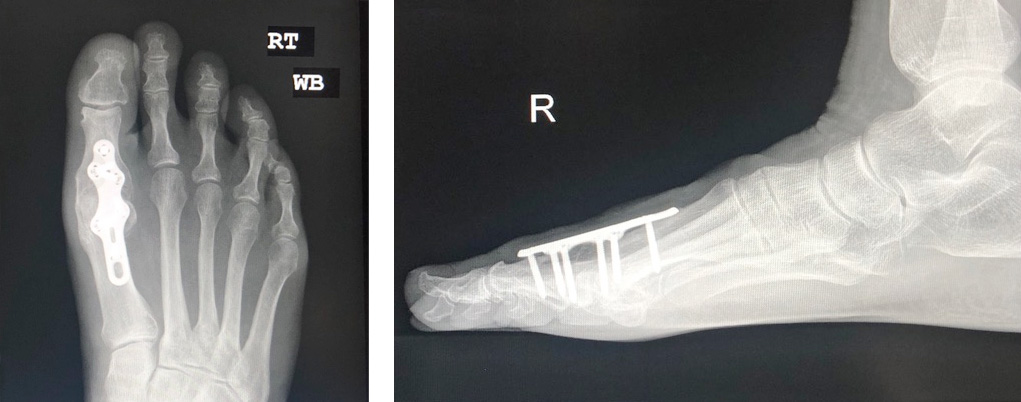
This operation removes the degraded part of the joint and fixes the joint together using a plate & screws, with the aim that new bone will grow across and 'fuse' the joint. It is perhaps the most successful operation in Foot & Ankle surgery and even in all orthopaedic surgery, with very high success rates and very low complication rates. The joint will then be rigid and no longer painful. Most people worry that the fused joint will cause problems - its extremely well tolerated and will allow nearly all sporting activities even to professional level! It does not alter normal walking obviously or visually.
MODERN LOW PROFILE TITANIUM PLATES ARE VERY STRONG AND ARE NOT PROMINENT. THEY PROVIDE EXCELLENT ALIGNMENT & FUSION RATES AND RARELY NEED TO BE REMOVED.
Preparation for Surgery
You should have received a letter detailing the codes and costs for the surgery and giving instructions on where to go and at what time. Please check these details carefully as you will be liable for any costs not covered by your insurers.
You will need to be nil-by-mouth – No food for 6 hours before surgery. Clear fluids (Water, Black tea or coffee / ribena ) can be taken for up to 2 hours before the operation.
MRSA status
Before or on admission to hospital a nasal swab will be taken to screen for MRSA. There is a small chance this is positive. If so your operation will be moved to the end of the list or rarely to another day to prevent cross infection.
Anaesthetic
The surgery is normally a daycase procedure, performed under a general anaesthetic with local anaesthetic (ankle block) after for additional pain relief. It is not normally a particularly painful operation and most patients report minimal pain.
Risks of surgery
Swelling
Initially the foot will be very swollen and needs elevating. The swelling will disperse over the following weeks & months but will still be apparent at 6-9 months.
Infection
There is always a risk of infection with surgery. The best way to reduce your chances of acquiring an infection is to keep the foot elevated for at least 10 days. You will be given 1 dose of intravenous antibiotics during surgery and if there there is an infection, it normally resolves with a course of oral antibiotics.
Malposition
The surgeon works hard to ensure the toe is fused in a position that allows optimum function and gives the best appearance. In the theatre we place your foot on a flat panel to simulate the normal standing posture of the foot. However, as you are asleep and lying down rather than standing with your whole weight on the foot, there is an element of experience and judgment in estimating the 'perfect' position. Occasionally, once the swelling has settled down, you may find the toe is fractionally higher or lower than before. This rarely causes a problem that requires further surgery and is usually accommodated with insoles.
Non Union
This is when the joint fails to fuse and bone has not grown across the joint. If this is painful then further surgery may be needed. The risk of this is approximately 10%.
Blood Clots
Because walking starts straight away there is no need for any anticoagulation. If you have at risk of blood clots please make us aware of this - you will be treated with an oral anticoagulants.
Immediately after surgery
Following surgery, the toe is protected in a specialised dressing and postoperative shoe.
You will be seen by a physiotherapist on the ward, who will advise on walking and early rehabilitation. You will be allowed home only when you are comfortable and capable.
Recovery from surgery
All things being normal, you can be discharged from hospital the same day, or the following day after surgery.
This type of operation and the post operative shoe allow weight bearing (walking) immediately. Often this may be too uncomfortable for the first week. Crutches are usually necessary for the first for 4-6 weeks.
The fusion must be protected with the specialised dressing for 2 weeks and you will need to wear a post operative shoe for 6 weeks.
Elevation of the foot (above the pelvis) for the first 10 days is vitally important to prevent infection. Naturally, small periods of walking and standing are necessary.Exercise: Static cycling and swimming can start after 4 weeks. Impact sports will take 4 months.
Swelling - many patients worry about the swelling. It is a natural response to the surgery and will take a 9-12 months to go.
Physiotherapy: This is not normally needed
Pain relief and take home medications
You will be given high doses of prescription painkillers to take home. Use these for the first 3-4 days and reassess.
Weight-bearing
You can walk on the foot immediately, in the protective shoe - the physiotherapist will assess and help you.
Washing and Bathing
It’s important to keep the dressing completely dry – the nurses will show you how to do this with a waterproof cover.
Activity and time off work
In general, up to 2 weeks off work is recommended if you have an office or sedentary job. Jobs or activities that involve a lot of standing or walking require a break of 6 weeks and more strenuous roles such as farming or construction where stresses are put on the joints, up to 8 weeks.
When can I start to drive again?
The DVLA states that it’s the responsibility of the driver to ensure they are always in control of the vehicle. Driving is allowed after 4 weeks on the right foot or 10 days on left foot for automatic cars. In both cases you will need to wear a shoe to drive in, as the post-op shoe is too big. It remains your responsibility to drive safely and you should also check with your vehicle insurer to confirm you are covered.
Results of surgery
Long term results of this type of surgery are excellent, with successful fusion rates of 95-100% in studies. (99% fusion in my own publication... Foot Ankle Int. 2010
First metatarsophalangeal arthrodesis using a dorsal plate and a compression screw. Kumar S, Pradhan R, Rosenfeld PF.