Extracorporeal Shockwave Therapy
Using focused high intensity sound waves to treat Plantar Faciitis & Achilles Tendinopathy
The potential of using high intensity sound waves as an effective a non-surgical treatment has been understood for quite a long time.
One of the earliest medical applications of high intensity sonic waves was in the non-surgical treatment of kidney stones (lithotripsy), where it was noticed that as well as being a very safe, non-invasive way of breaking up the stones, the effect of the shock waves on surrounding tissue also had the effect of reducing inflammation and stimulating the formation of new blood vessels, which in turn helped dissolve calcium deposits.
What is the science behind it?
Just like an ultrasound scan, ESWT uses a gel to carry the waves from a transponder into the tissue. The process works by focussing the sound waves at a point where they have a direct mechanical effect deep in the tissue. Energy is released via 'bubble cavitation'. If you like, think of it as a deep, strong and precise means of directing a massage to a point well beyond the reach of a physiotherapists fingers. (Seil R et al Extracorporeal shock wave therapy for tendinopathies. Expert Rev Med Dev 2006;3:463-470))
Interestingly, shockwave therapy also has a direct effect on neurones in the area being treated, particularly sensory nerves that carry pain signals. Experiments have shown there can be a reduction in the number of pain carrying nerve fibres in the treated area. (Ohtori et al, Neurosci Lett 2001 ;315;57-60)
Another important effect comes from evidence that shows an increase in the production of growth factors in animal tendons treated with ESWT. Tendons are often slow to heal and recover from injury, so this is an important benefit. (Chen et al, J Orthop Res 2004;22:854-861)
There is also strong evidence that it promotes new blood vessel growth (angiogenesis) around the tendon bone junction – which is the point where the majority of these painful conditions develop. (Wang et al, J Orthop Res 2003;21:984-989)
Chronic Heel Pain – the where and why
Many people suffer from chronic heel pain at some point, either through injury or the natural effects of ageing. In few but the most serious of cases would surgery be required or even advisable.
That said, it is a very debilitating condition that effects quality of life and deserves serious and considered medical investigation and treatment.
There are two classic types of heel pain and occur at different areas. Heel pad pain, often called 'policemans heel', or heel bump pain at the back. There are several causes of both types and its important to identify this precisely to give the best treatment.
The classic 'Policeman's Heel' presents as a pain under the heel pad, similar to the feeling of a bruise caused by treading on a small stone. It tends to be worse in the morning or after periods of sitting down and you may find yourself hobbling.
Causes
- Plantar fascitits – effectively Tennis Elbow of the heel. This is the most common cause (95%). Inflammation and degeneration of the plantar fascia where it inserts on to the heel. The PF is a strong ligament that supports the arch of the foot.
- Tarsal Tunnel syndrome – next most common cause
- Stress fracture of the calcaneum. There is no need for an injury. May be a sign of underlying bone weakness and hormone deficiency.
- Inflammatory conditions – may be part of a rheumatological condition
- Lower back problems. Rarely the individual nerve to the heel is trapped in the back. S1 nerve root.

Severe Plantar Fasciitis
Diagnosis
Careful and precise examination will identify the common causes. MRI or nerve test can be undertaken if cause is uncertain…
Treatment
a. Physio – Achilles & PF stretches
b. Cushioned or custom made insoles
c. Shockwave therapy. Ta da!
This treatment has transformed the recovery from this condition.
There is now a large body of scientific evidence and clinical experience to support the benefits of ESWT in both Plantar Fasciitis and Achilles Tendinopathy.
A paper in The American Journal of Sports Medicine, 2008, Vol. 36, No. 11, 2100-2109 by L Gerdesmeyer et al. found that shockwave therapy significantly improved pain, function and quality of life in patients with chronic plantas fasciitis, with a 61% success rate after 12 weeks and higher after 12 months.
A survey conducted by a the distributor of ESWT systems found that:
90% of doctors rated treatment of plantar fasciitis as good or very good
87% of doctors rated treatment of Achilles tendonitis as good or very good
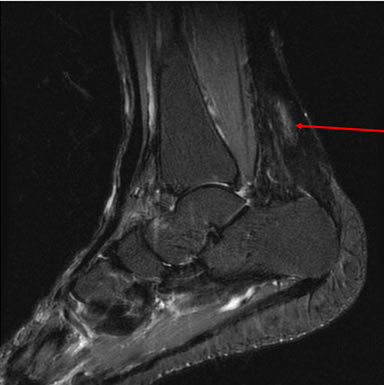
Achilles tendon
Whilst professional sportspeople and the unfortunate few may occasionally rupture their Achilles tendon, the rest of us are more likely to have a combination of inflammation and calcification of the tendon which leads to pain and stiffness. In Achilles tendinopathy you'll usually feel this pain at the back of the heel above where the tendon attaches to the bone. Although there is a slight variation where the pain occurs just at the point where it meets the bone. It can be stiff in the morning and wear off a little once the tendon 'warms up'.
No waiting, no hospital, no complications, completed in 15 minutes.
In most cases, first port of call with both of these conditions is to work with a physiotherapist on stretching exercises and possibly the adaptation of footwear. Stretching the tendon and something as simple as heel pads or different types of footwear can be highly, sometimes surprisingly, effective.
1. LOCATING PAIN BY PALPITATION

2. MARKING THE AREA TREATMENT

3. APPLYING THE CONTACT GEL

4. DELIVERING THE SHOCKWAVES

However, where the pain proves intractible with conservative treatments, a thorough clinical history and examination - perhaps requiring an x-ray or ultrasound scan, will indicate whether shockwave therapy alone or in combination is indicated.
Modern doppler ultrasound scanners give a detailed picture of the blood flow around the tendon, showing areas of 'neovascularity' where new blood vessels are forming. These areas of vascularity can contribute to continuing inflammation and may require treatment with steroid injections.
The ESWT Treatment
A typical course of treatment will require 3 to 5 sessions, conducted no more than 2 weeks apart.
It can take up to 3 sessions or 12 weeks for the effect of ESWT to be apparent, but many patients notice an improvement very quickly.
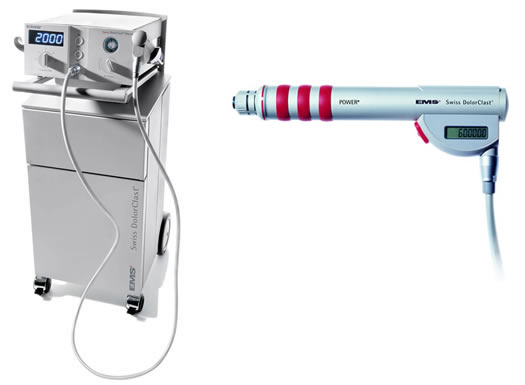
Treatments are conducted at the clinic by me. Each session takes around 10 minutes and you lie on your front while the shockwave is applied. We use the state of the art Swiss DolarClast system and the waves are directed using an attachment that looks not unlike something you'd use for DIY.
As we are pressing on a sensitive area and the shockwaves themselves are having a mechanical effect, some local anaesthesia may be required or desired. Certainly, a degree of discomfort during the procedure is normal and it not unusual for heel pain to become slightly worse immediately after treatment before getting better.
My experience is that the treatment works well for around 80 per cent of patients and the effect is long term and often permanent.
For more information on shockwave therapy, you can also read the following.