Bunion Information & Types
What is a bunion?
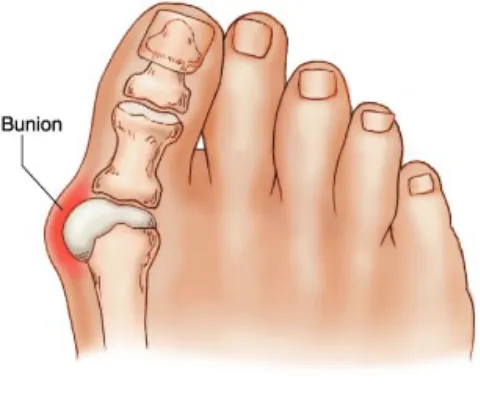
A bunion is a bony lump that forms on the side of the big toe joint. It develops due to a prominent bone (the metatarsal head) and thickened overlying soft tissue. As the bunion progresses, the big toe often deviates outward, a condition known as Hallux Valgus. This misalignment can lead to pain, swelling, and difficulty finding comfortable footwear. Over time, the joint may become stiff and arthritic, further limiting movement and increasing discomfort.
Why does it happen?
The primary cause of bunions is genetics. If a parent or grandparent had bunions, there is a significant chance of inheriting the predisposition. However, environmental factors also contribute to their development. Tight, narrow, or high-heeled shoes that compress the toes together can exacerbate the problem by stretching the ligaments and altering foot biomechanics.
Bunions are significantly more common in women, largely due to footwear choices and structural differences in foot anatomy. They are also more prevalent in individuals with flat feet, as the altered foot mechanics place additional stress on the metatarsal joint.
Hallux Valgus and bunions affect approximately 23% of adults aged 18-65, and prevalence increases to 35.7% in individuals over 65. As people age, the likelihood of developing bunions increases due to gradual weakening of ligaments and continued exposure to weight-bearing stress.

How do I prevent it?
Shoeware
The best way to prevent a bunion forming is to wear shoes that fit the natural shape of the forefoot, and do not squash the toes together. There is no other reliable treatment as it is an inherited problem, but arch supports can make the foot more comfortable and may be of benefit, particularly in people with flat feet.
Toe spacers and braces
There are many makes of bunion straps and night splints available commercially. These may make the toe more comfortable while worn, but do not reverse it or prevent them getting worse.
Stretching and strengthening exercises
Specific exercises aimed at improving foot and toe flexibility may help slow progression and reduce pain. Strengthening the small muscles of the foot can enhance stability and provide additional.
Are they all the same?
The term “Bunion” covers many different types of problem and there is a range of deformities and treatments.
Simple bunion
Due purely to a bony prominence on the side of the metatarsal head - there is no deformity in the toe or the metatarsal. If wider shoes don’t work, they can be treated with Minimally Invasive Surgery (MI) - this is the least invasive surgery and has the quickest recovery.

Hallux valgus
The most common type, where the metatarsal bone deviates outwards and the toe deviates inwards. As the bones become angled, the ligaments on the inside of the joint stretch (medial capsule) and the muscles on the other side contract, pulling the toe over (adductor hallucis muscle).
The surgery to correct this is more involved and requires careful appreciation of all the contributing factors. The metatarsal is cut and realigned, the tight muscles and tendons are released and cut and the stretched ligaments reconstructed and tightened. This can be done with MI surgery or open surgery depending on the exact type of problem. (For further information see the surgery section on hallux valgus corrections).



Severe Hallux valgus with lesser toe deformities
In more severe cases, the Hallux Valgus causes deformity in the lesser toes too. These become clawed and painful underneath (“Metatarsalgia”) and eventually crossover the hallux.
These require the most complex surgery, with realignment of the hallux / metatarsal and correction of the clawed toes. This involves realignment of the Hallux metatarsal as above, or fusion of the joint (see MTP fusion), combined with shortening of the lesser metatarsals (DMMO), with fusions of the small joints of the toes (interphalangeal joint fusions). This may be combined with ligament reconstruction of lesser toes (plantar plate reconstruction) and tendon lengthening or reconstruction. The surgery is complex, uses a combination of open and MI techniques and can take 2 hours or more.

Do bunions get worse?
Bunions usually get worse, slowly, over many years. There is a gradual increase in the deformity and usually with pain. This can be interspersed with long periods when the toes and foot are ‘quiet’, with the deformity and pain resting.
Over time, there is a slow migration of the big toe inwards. As it does so, it takes less and less body weight (biomechanical underload) and the lesser toes take more weight (biomechanical overload). This causes “metatarsalgia” - pain underneath the ‘ball’ of the foot, which feels like there is a “pebble in the shoe”.
As this overload continues, the toes become clawed - bending at the IP joints (interphalangeal joints) and becoming lax and unstable at the MTP joints (metatarsophalangeal joints). This is due to stretching of the ligament that supports the joint (plantar plate).
Rarely, this process can suddenly accelerate, with a rapid change in the deformity and symptoms.

When is surgery indicated?
In early or mild cases, surgery can usually be avoided. In general, the majority of symptoms from a minor deformity can be controlled by correctly fitting shoes or insoles.
If the correct shoes / insoles do not control the pain, then surgery is indicated. There is normally no need to rush ahead with surgery and it can be organised to fit in with your schedules and timetables.
If the hallux valgus becomes unstable, with a sudden increase in the deformity or there are signs of clawing of the toes, then earlier surgery is usually needed. The progression in the deformity will continue, requiring more complex surgery and the worse it is, the harder it is to get right.
In more severe cases, shoes and insoles will still help with the pain, but surgery is usually necessary to achieve maximal relief.

Bunion Surgery - what does it involve?
The principles behind the surgery are to realign the bones (osteotomy) and to correct the ligaments and stretched tissues.
Prior to surgery, the foot deformities and xrays need precise assessment. No bunion is the same, and there is a complex interplay between the bone deformities and soft tissue contractures.
This needs careful assessment to decide upon the correct operation and to achieve the goal of a comfortable straight foot. No single operation caters for all bunions and the results will be below standard if the wrong procedure is used.
Recovery
The recovery from bunion surgery is more prolongued than one might expect. This is due to the swelling which takes months to dissipate. Often the foot remains too swollen to fit into normal shoes for 9-12 weeks. It will be 4-6 months before you are walking long distances in comfort. Therefore, it is sensible to leave 4-5 months before any special or major occasions.
Anaesthesia
The surgery is performed routinely as a daycase, under general anaesthesia with a regional anaesthetic (ankle block) for pain relief. The patients are discharged the same day, fully weightbearing in a protective shoe. No plastercast is necessary.
Are there any risks of surgery?
Of course there are risks with any operation. The more frequent risks and complications are of bunion surgery are outlined and discussed in the operative sections.
When should I have surgery?
Surgery is rarely essential and more accommodative shoeware should be tried first. Unfortunately, toe-spacers, braces and orthotics do not help in the long term. Custom made shoes can be very good for severe cases where surgery is contra-indicated.
The timing of surgery and when to recommend it is a common quandary. In a stable situation, when there has been no change in deformity or symptoms, wider more accommodative shoes can help. In an unstable situation, when the pain or deformity is increasing or there are changes to the lesser toes (clawing or metatarsalgia), surgery should be considered. If left, the deformities will get worse, making surgery more complex and more extensive and previous studies have shown that surgery in these cases do less well, with higher complications and recurrence rates.
The results of modern surgery are substantially better, with published satisfaction rates of 94% (Adam 2011). This improvement is due to advances in surgical techniques, with the modern types of osteotomy and screw fixation providing a more stable construct. This reduces the surgical pain and allows immediate weightbearing. New techniques provide more precise bony realignment and balancing of the soft-tissues, with greatly improved immediate and long-term corrections. The latest advances in minimally invasive surgery further reduce surgical trauma, infection rates and recovery times.
The surgery is performed routinely as a daycase, under anaesthesia with a regional anaesthetic (ankle block) for pain relief. The patients are discharged the same day, fully weightbearing in a protective shoe. No plastercast is necessary. They have improved recovery, reduced pain, immediate weightbearing and early return to work.
The recovery from bunion surgery is more prolongued than one might expect. This is due to the swelling which takes months to dissipate. Often the foot remains too swollen to fit into normal shoes for 9-12 weeks. It will be 4-6 months before you are walking long distances in comfort. Therefore, it is sensible to leave 4-5 months before any special or major occasions.